|
|
|
Home | Clinical Background and Need | Engineering Principles and Clinical Considerations | Commercial Devices | Upcoming Advancements |
|
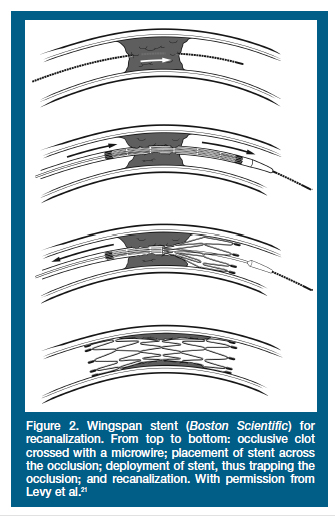
Upcoming Advancements Stent Assisted Recanalization in Acute Ischemic Stroke Initial clinical stent-assisted intracranial recanalization utilized coronary stents with balloon deployment after conventional drug and mechanical approaches had failed. Five self expanding stents designed for the cerebrovasculature are currently available, four of which (Neuroform, Boston Scientific; Enterprise, Codman Neruovascular; Leo, Balt Extrusion; Solitaire/Solo, EV3) are marketed for stent assisted coil embolization of aneurysms, and one of which (Wingspan, Boston Scientific) is marketed for treatment of symptomatic intracranial atherosclerosis. Self-expanding stents are deployed with significantly lower forces compared to balloon-mounted coronary stents; because most cases of stroke are due to an embolism causing an obstruction in a location without in situ vascular pathology, ballon angioplasty and balloon-expandable stenting is overkill. Self expanding stents may cause less endothelial damage compared to balloon-expandable stents, which may lower rates of restenosis. Currently, the Wingspan stent is being tested in a Phase II FDA HDE (Humanitarian Device Exemption) clinical study. The Wingspan is only used as a last resort after failure of current FDA-approved recanalization methods. The longest length of the Wingspan stent is 20 mm, so only patients with a clot measuring 16 mm or less are candidates. The access site is either the femoral or radial artery. A guide catheter is placed in the target vessel proximal to the occlusion. First, a guidewire is advanced through the distal end of the guide catheter and beyond (distal to) the blockage. Then a microcatheter is advanced over the guidewire through and beyond (distal to) the blockage. To minimize risk of distal embolism, the guidewire and microcatheter are advanced between the vessel wall and the thrombosis without making contact with the thrombosis. An exchange wire is then advanced through the microcatheter and anchored distal to the blockage. The microcatheter is retracted, and the stent delivery catheter is advanced over the exchange wire. The stent is deployed, starting distal to the blockage and ending just proximal to the blockage. This distal deployment methodology minimizes distal embolism because debris that is released as the stent is deployed through the blockage is trapped by the already deployed portion of the stent distal to the blockage. If the stent is not expanded to at least half of the vessel diameter, an angioplasty balloon is used to slowly expand the stent to the appropriate diameter. Figure 1 summarizes this procedure.
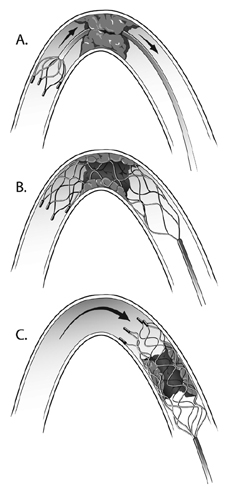
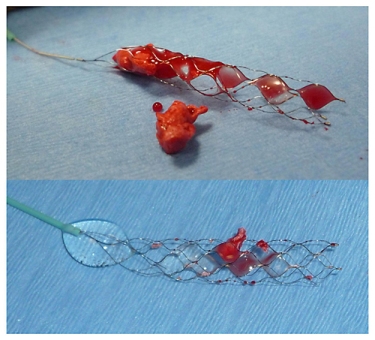
Figure 1. Stenting of atherosclerotic or occluded intracranial vessels (1). Generally positive results are shown in retrospective studies using Neuroform, Wingspan, and Enterprise stents for recanalization in the acute stroke setting, both alone and with adjunctive drug or FDA-approved mechanical thrombectomy techniques/devices. These devices were used as last-resort when these FDA-approved therapies did not succeed in recanalization. In 193 patients treated for acute ischemic stroke, there were 52 (26.9%) patients who underwent stent assisted recanalization after failed recanalization attempts with FDA-approved therapies. A Thrombolysis In Myocardial Infarction Grade of 2 or 3 was achieved in 71.2% of these patients. Patient outcomes at 3 months were mean Rankin Scores less than or equal to 2 in 42.3% of these patients and mortality rate of 21.2% in these patients. Restenosis was not observed at 3 months. Limitations include difficulty in stenting smaller vessels and inability to stent clots that are longer in length than the stent or located at bifurcations. Antiplatelet drug use must be continued for 3 to 6 months after stent placement. Another limitation is that the stent is typically a permanent implant in the vessel; more 'traditional' mechanical thrombectomy techniques do not leave a permanent implant behind. Additionally, restenosis in the stent is possible and observed: mid-term results for the Wingspan stent implanted to treat atherosclerotic intracranial stenosis show a 25 to 29 % restenosis rate. Stent assistance can be used for temporary endovascular bypass as well. Closed-cell stents are able to be partially or fully deployed and then recaptured. Thus, they can be partially or fully deployed to achieve immediate blood flow restoration while other mechanical thrombectomy techniques are used to remove the thrombosis. Once the thrombosis is removed, the stent can be resheathed and removed. This obviates the need for many dual antiplatelet therapies, gives the interventional radiologist more time for thombectomy, and eliminates the long-term risks of a permanent implant. The Enterprise stent and the Solitaire FR stent have been used in this fashion. The Solitaire FR stent is a fully recoverable, self-expanding thrombectomy device that was based on the Solitaire/Solo stent. The Solitaire FR can be used either as a temporary endovascular bypass or as a permanent implant via electrolytic detachment (1). A balloon guide catheter is placed proximal to the blockage site. The blockage is crossed (between the vessel wall and the thrombosis) with a guidewire by advancing the guidewire through the balloon guide catheter. A microcatheter is then tracked over the guidewire until it is distal to the blockage. The guidewire is then retracted and the Solitaire FR system is advanced through the microcatheter until the entire length of the Solitaire FR stent is distal to the blockage. The balloon is then inflated to occlude antegrade blood flow. The Solitaire FR is then deployed until the distal marker of the microcatheter is aligned with the proximal marker of the stent (Figure 2 parts A and B). The deployed stent and microcatheter are then retracted simultaneously as one unit through the balloon guide catheter while constant aspiration is performed on the balloon guide catheter with a syringe (Figure 2 part C). Figure 3 shows a thrombosis removal in a canine stroke model (2).
The Solitaire FR With the Intention for Thrombectomy (SWIFT) study is currently recruiting participants to demonstrate equivalence of the Solitaire FR device to the Merci Retrieval System. The study aims to demonstrate the safety and efficacy of the Solitaire FR for providing mechanical thrombectomy treatment to patients with acute ischemic stroke (3). (3) SOLITAIRE™ FR With the Intention For Thrombectomy (SWIFT) Study from ClinicalTrials.gov
|