|
||
Spinal fusion has been the treatment of choice for symptomatic DDD that has not responded to conservative treatment modalities, however, immobilization of the fused spinal segment can cause increased stress at adjacent segment levels, potentially furthering the DDD process[4].
Artificial Disc Replacement, is a surgical procedure in which degenerated intervertebral discs in the spinal column are replaced with artificial ones [5]. Artificial disc procedures were developed with the goal of pain reduction or elimination, while still allowing motion throughout the spine. Another advantage is the prevention of premature breakdown in adjacent levels of the spine, a potential risk in fusion surgeries.
Key Design Features
A variety of factors designers to be followed when designing an artificial disc. The device must be able to maintain proper intervertebral spacing, allow for the full range of motion and provide stability. Like a natural disc, the artificial disc must act as a shock absorber. Finally, the artificial disc must be very durable. The average age of a patient needing a lumbar disc replacement is about 35 years. This requires the device need to endure more than 1 million times of bending cycles over the 50-year life expectancy of the artificial disc. Another important issue is the materials should be biocompatible, that are safe to be implanted in the human body, not cause allergic reactions and not damage other parts of the spine.
The World's First Artificial Disc
The pioneer should be the CHARITE Artificial Disc, which was originally developed at the CHARITE?University Hospital?in Berlin, Germany in the mid-1980's by Prof. Karin Büttner-Janz, and Prof. Kurt Schellnack. Further refinements to the design were incorporated with the cooperation of the staff at Waldemar Link GmbH, a leading European based medical device manufacturer. After years of effort, FDA approved the CHARITE Artificial Disc in October of 2004 after extensive review of the two year U.S. clinical trial results. In addition to these studies, total disc replacement with the CHARITE Artificial Disc has been performed in Europe for over 17 years.
 |
 |
| Figure 1. CHARITE Artificial Disc (DePuy Spine, Inc.) | Figure 2. Replacement Scheme |
Current Artifical Disc Types and Models
Composite Discs
The most widely implanted disc to date is a composite disc. This device is made of a polyethylene spacer and two separate metal endplates and comes in different sizes. It also has a ring around it to make it visible on an x-ray.
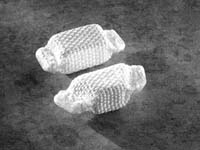
Hydraulic Artificial Discs
Hydraulic artificial discs have a gel-like core covered with a tightly woven polyethylene "jacket". Before it is implanted, the pellet-shaped hydrogel core is compressed and dehydrated to minimize its size. Once it is implanted, the outer woven covering allows fluid to pass through to the core, which immediately begins to absorb fluid and expand.
Elastic Discs
Elastic type artificial discs are made of a rubber core bonded to two titanium endplates.
Mechanical Discs
Several pivot or ball type artificial discs have been developed for the lumbar spine. One device, made of metal-hinged plates with an interposed spring, has been tested on sheep with good results. Another device has a polyethylene core and metal endplates with two vertical wings. Patients who received this implant reported good to excellent results.
 |
 |
 |
 |
| 1.The Bryan Artificial Disc | 2.The PDN Prosthetic Disc Nucleus | 3.The Acroflex Disc | 4.The Prestige Disc |
Current Limitations and Future
-
Limited patients physical movement during the recovery
-
Mechanic property
-
Lifespan and biocompatibility
Disc replacement is technically challenging and for many surgeons will involve a major change in their usual operative practice. All current discs are placed through the anterior approach, making most spine surgeons will require an access surgeon. Developing minimal invasive technology should be taken into consideration to decrease patients' inconvenience and surgery time.
All other arthroplasties have demonstrated a finite lifespan. Patients undergoing disc arthroplasty will be much younger (30s to 50s) and revision anterior surgery at the lower lumbar level is very difficult. Therefore, implant longevity is of vital importance.
Artificial spinal disc replacement is not only possible but it has been the potential of revolutionizing the treatment of spinal degeneration. We have every reason to believe this technology can provide relief to millions of back pain sufferers and bring their quality life back. Engineering better health, the future is brighter!