 |
|||||||||||||||
|
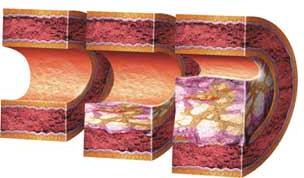
Clinical BackgroundThis section discusses the clinical relevance of drug-eluting stents, including a brief description of coronary artery disease and a history of the progression of coronary stents. Coronary Artery DiseaseCoronary artery disease occurs when plaque builds up in the arteries, thus narrowing the lumen of the arteries and decreasing blood flow to the heart. This plaque is essentially a build-up of cholesterol (or fat) within the artery wall. The process of hardening of the coronary arteries is known as atherosclerosis. The patient begins to develop symptoms of obstructive coronary artery disease once plaque begins to block more than 70% of the lumen of the artery. Arteries which are narrowed beyond this point may have trouble delivering oxygen-rich blood to tissues, which results in myocardial ischemia. If the plaque ruptures, a myocardial infarction (or heart attack) may occur. A diagram of the progression of coronary artery disease is shown below (Figure 2).
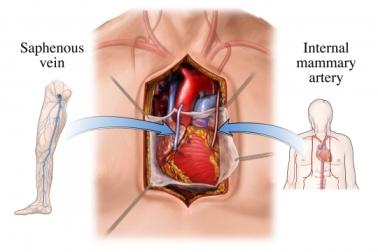
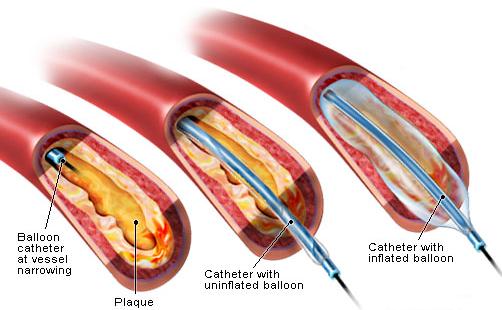
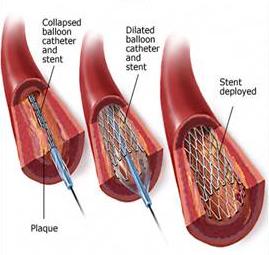
History of StentsA timeline of the progression of treament options for coronary artery disease is shown and described below. - 1960's: Coronary Artery Bypass Graft (CABG) Coronary Artery Bypass Grafts (CABG's) were developed in the 1960's to treat coronary artery disease. A vein from the patient's body, typically the saphenous vein from the leg, is harvested. It is then transplanted around the narrowed sections of the coronary arteries to create a "bypass" for blood to flow. Even though this procedure has a high success rate, it is very invasive and requires open heart surgery. - 1970's: Percutaneous Transluminal Coronary Angioplasty (PTCA), a.k.a. Balloon Angioplasty Percutaneous Transluminal Coronary Angioplasty, better known as Balloon Angioplasty, was developed in the 1970's. A catheter is inserted percutaneously into the patient's body through a peripheral artery. A balloon at the end of the catheter is then inflated at the site of the blocked arteries. The balloon may be inflated and deflated several times to compress the plaque and create an opening in the narrowed artery. This technique has a high rate of restenosis (about 40%), but is much less invasive than a CABG procedure. - early 1990's: Bare Metal Stents Bare Metal Stents were created in the early 1990's to attempt to alleviate the problem of restenosis. An expandable wire mesh is placed around the balloon in a Balloon Angioplasty procedure. The stent is inserted through a peripheral artery to the diseased artery, very similar to balloon angioplasty. The metal stent is then left behind at the site of the blockage once the balloon is inflated. The purpose of this stent is to hold open the artery. The restenosis rate using bare metal stents is about 25%. - late 1990's: Drug Eluting Stents In the late 1990's, Drug-Eluting Stents were created to again address the problem of restenosis. The use of drug-eluting stents is the current and most widely used procedure to treat coronary artery disease. It is estimated to reach utilization in 87% of stent procedures today. This website describes drug-eluting stents, and its impact on the treatment of coronary artery disease. A timeline of the evolution of coronary artery disease treatments (coronary artery bypass graft
Next: Current Devices
|
Home![]() Clinical
Background
Clinical
Background![]() Current Devices
Current Devices![]() Future
Research
Future
Research![]() References
References
Website by
Ken Cheng![]() UC-Irvine, BME240
UC-Irvine, BME240![]() This site was last updated
06/12/07
This site was last updated
06/12/07
![]()