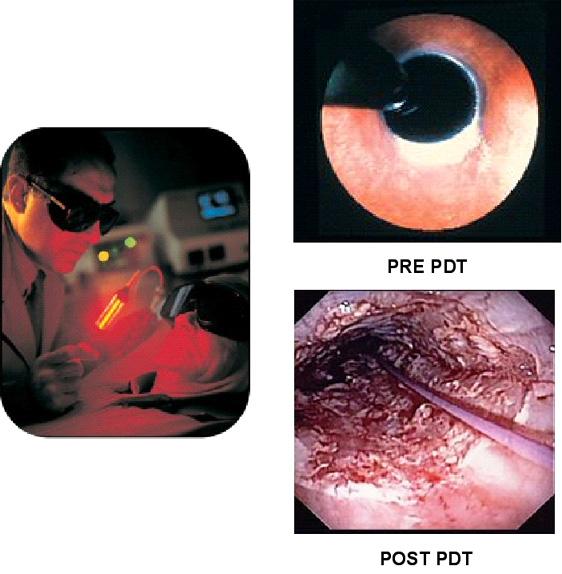
Photodynamic therapy
(PDT) is a treatment that uses a combination of a photosensitizer (a
light activated drug) and a laser light to destroy abnormal cells. The
primary use of PDT is as an alternative to esophagectomy (the surgical
removal of the esophagus) for patients with high-grade dysplasia (HGD)
and early cancer in Barrett's esophagus.
The first step in PDT
involves the administration of a chemical photosensitizer, some of which
becomes concentrated in the abnormal esophageal mucosa (5-aminolevulinic
acid) and some in the stroma (porfimer sodium). The only approved
photosensitizer in North America is porfimer sodium (Photofrin® [Axcan
Pharma Inc, Birmingham, AL]), which is given intravenously. Laser light
is then delivered two-three days later using a specially designed light
delivery balloon. Activation of the photosensitizer by an
endoscopically applied light source at the appropriate wavelength (630
nm for porfimer sodium) induces the generation of singlet oxygen
and other cytotoxic species that contribute to the destruction of the
abnormal esophageal mucosa, resulting in deep injury that is associated
with significant morbidity (11). Photofrin remains in the skin for up to
2 months and thus the patients must avoid direct exposure to sunlight
and bright lights during this time, since exposure to light may result
in severe sunburn (12).
Overholt et al. have published extensively
regarding their experience of using PDT in 103 patients, most of whom
had HGD. The mean follow-up in this group was over 4 years. Of the 65
patients with HGD, 78% had their HGD eliminated. On the basis of an
intention-to-treat analysis, 54% had no residual Barrett Esophagus. The
primary complication of PDT for Barrett's esophagus is esophageal
stricture, scarring and narrowing of the esophageal lumen. The overall
stricture rate for patients treated with PDT was 30%, but for those who
required more than one PDT treatment it was 50%. Such strictures are usually responsive to
endoscopic balloon dilation. Another
important finding in patients undergoing PDT with apparent squamous re-epithelialization
is the presence of residual patches of subsquamous intestinal metaplasia. Subsquamous, nondysplastic intestinal metaplasia occurred in 4.9%
of patients, but more importantly 3 patients (4.6%) developed
subsquamous adenocarcinoma (13). The occurrence of subsquamous
intestinal metaplasia is reported in virtually all studies using PDT: in
detailed pathology studies the prevalence is reported to be as high as
51.5% (14). Other side effects reported with PDT include chest pain,
dysphagia, odynophagia, pleural effusions,
Candida esophagitis, and atrial fibrillation. In addition, esophageal perforation and
tracheoesophageal fistulas have been reported, but are rare (<1%) (15).
Esophagectomy remains the gold standard
treatment for HGD. As techniques and technology improve, it is likely
that ablative strategies will become an important part of the
armamentarium in the treatment of Barrett’s esophagus (16). A recent
cost-effectiveness analysis of PDT for HGD in Barrett's esophagus found
PDT to be a cost-effective alternative to esophagectomy, even though it
incurs the greatest lifetime cost (US $47,310) compared with
esophagectomy (US $24,045) (17).