Gastroesophageal reflux disease (GERD) is a
condition which results from the chronic reflux of gastric contents into
the lower esophagus. GERD is caused by a decreased efficacy of
esophageal anti-reflux mechanisms, particularly a decrease in LES tone.
Normal LES pressure is 10-15 mmHg, a decrease LES tone leads to a
decrease in LES pressure and thus a lower gastric pressure is required
to break through the barrier and cause reflux of the positively
pressured gastric contents into the negatively pressured esophagus.
GERD typically occurs when LES pressures are <10 mmHg (2). Long-term
esophageal pH and manometry studies have revealed another contributory
mechanism to GERD pathology related to transient LES relaxations (TLESR).
The TLESR are physiological and thus the esophagus will be exposed to
small amounts of acid in a healthy person following meals. However, in
patients with GERD the frequency and duration of TLESR are increased,
therefore increasing the risk of symptoms and esophageal damage (3).
CNS depressants, hypothyroidism, pregnancy, systemic scleroderma,
alcohol use, tobacco use are well known contributing causes to GERD.
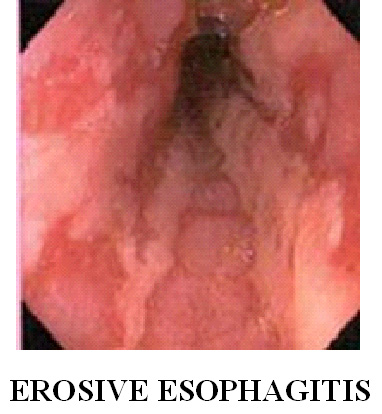
However, in most cases no antecedent etiology is identified. The low pH
of the gastric contents that are refluxed into the esophagus leads to
esophageal mucosal injury, i.e., erosive esohpagitis. The clinical
symptoms associated with GERD are dysphagia, heartburn, and
regurgitation. Rarely chronic symptoms are associated with attacks of
severe substernal chest pain which may be mistaken with a heart attack.
The potential consequences of GERD are hemorrhage, ulceration, stricture
formation, and the dreaded development of Barrett esophagus.
Anti-reflux therapy is designed to eliminate the
signs and symptoms of GERD and to prevent its complications. Both anti-secretory
therapy (H2-blockers, PPIs) and surgical fundoplication have been shown
to be effective in reducing or eliminating reflux symptoms. Despite
excellent control of symptoms, no anti-reflux therapy has been
definitively proven to promote the regression and/or prevent the
progression of Barrett's metaplasia or to decrease the risk of
esophageal adenocarcinoma (4).