 |

Current Techniques
What treatments exist for stones?
Observation - Smaller stones (approximately 5 mm in size or less) can be followed and given an opportunity to pass spontaneously.
ESWL - Extracorporeal shock wave lithotripsy utilizes shock wave energy traveling through water to fragment a stone. The stone fragments are then allowed to pass independently or are retrieved with endoscopic measures.
 |
 |
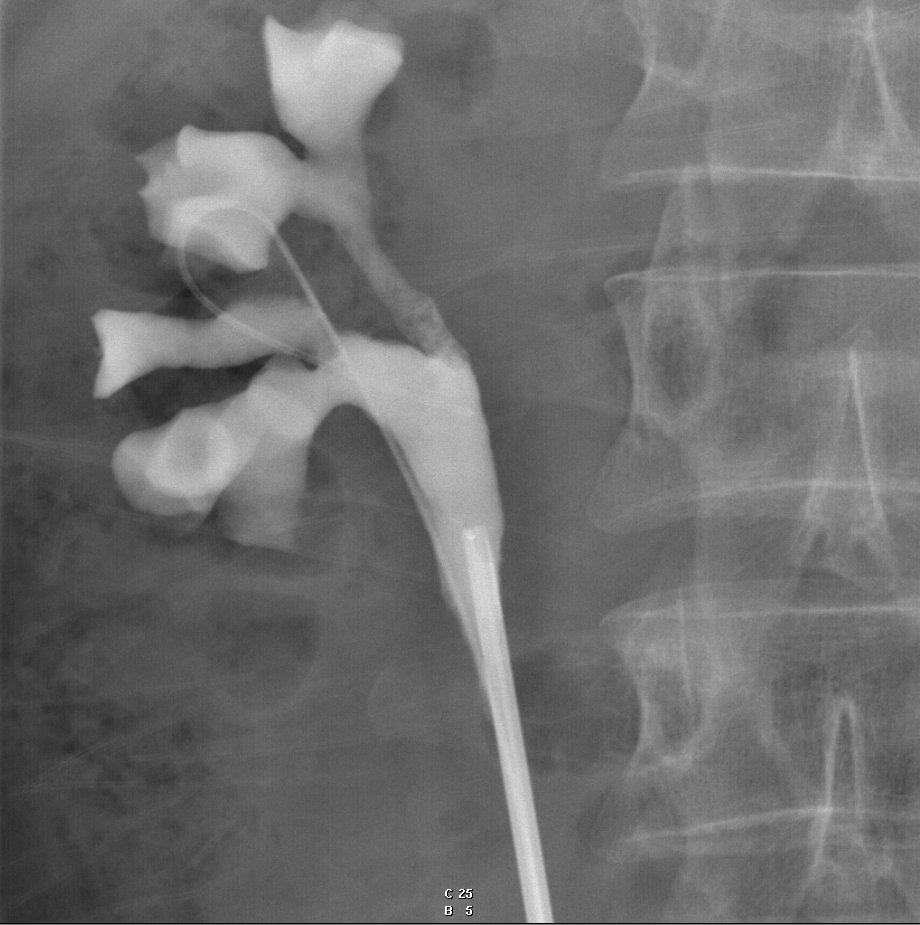
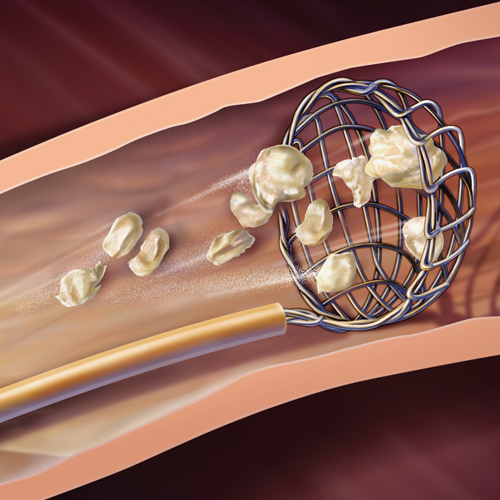
Endoscopic Procedures - These procedures use minimally invasive technology to localize a stone, fragment it with an energy source when necessary (i.e., laser), and then retrieve the fragments. Endoscopes with magnifying cameras are advanced into the drainage system of the urinary tract in order to facilitate stone fragmentation and retrieval.
 |
 |
Other Surgical Procedures - Rarely, it is necessary to utilize laparoscopic or traditional open surgery in order to treat urinary tract stone disease. Recently, endosurgical mechanical cystolithotripsy followed by percutaneous extraction has been evolved for small or moderate-sized calculi. It has an added advantage as it can be combined with a corrective procedure for bladder outlet obstruction. Electrohydraulic shockwave lithotripsy (EHSWL) is preferably to be avoided in hard, large vesical calculi and if the stone is in a diverticulum or stuck to the mucosa.
Medical Therapy - Certain stones can be treated with medications in order to help them dissolve. In particular, uric acid and cystine stones may be treated by a process known as alkalinization of the urine. Additionally, fluid consumption, dietary intake, and medications can be used to prevent stone recurrences in patients who are likely to form stones.
How can we prevent stones formation?
Measures to prevent the formation of new stones vary, depending on the composition of the existing stones.
 |
Drinking large amounts of fluids—8 to 10 ten-ounce (300-milliliter) glasses a day—is recommended for prevention of all stones, although it is not clear whether and how much this helps. Many people with calcium stones have a condition called hypercalciuria, in which excess calcium is excreted in the urine. For them, a diet that is low in sodium and high in potassium may also help. Calcium intake should be about normal, 1000 to 1500 mg daily. Restricting dietary protein from red meat may help reduce the risk of stone formation. Thiazide diuretics, such as chlortalidone or indapamide, reduce the concentration of calcium in the urine and help prevent the formation of new stones in such people. Potassium citrate may be given to increase a low urine level of citrate, a substance that inhibits calcium stone formation. |
Many people with calcium stones have a condition called hypercalciuria, in which excess calcium is excreted in the urine. For them, a diet that is low in sodium and high in potassium may also help. Calcium intake should be about normal, 1000 to 1500 mg daily. Restricting dietary protein from red meat may help reduce the risk of stone formation. Thiazide diuretics, such as chlortalidone or indapamide, reduce the concentration of calcium in the urine and help prevent the formation of new stones in such people. Potassium citrate may be given to increase a low urine level of citrate, a substance that inhibits calcium stone formation.
A high level of oxalate in the urine, which contributes to calcium stone formation, may result from excess consumption of foods high in oxalate, such as rhubarb, spinach, cocoa, nuts, pepper, and tea, or from certain intestinal disorders. Calcium citrate, cholestyramine, and a low-oxalate, low-fat diet may help to reduce urinary oxalate levels in some people. Sometimes pyridoxine decreases the amount of oxalate the body makes.
 |
Web Design by Ylenia Santoro |
