Home Wound Healing Literature Review Strategy References
|
Home Wound Healing Literature Review Strategy References |
 |
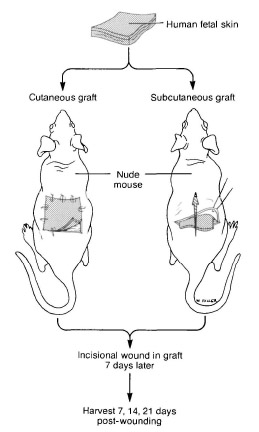
Review of Relevant Literature In contrast to wound healing in cutaneous tissue, wounds in the oral mucosa show privileged healing; they remodel quickly, and undergo reepeithelialization with minimal scar formation. In these respects, wound healing in the oral mucosa is similar to fetal cutaneous wound healing during the early gestational period, in which wounds also heal quickly with little or no scar formation. Wounds in the oral mucosa contract quickly to reduce wound size, which is in contrast to cutaneous wounds, in which contraction accounts for a small fraction of wound closure. The myofibroblast, formed from differentiation of resident fibroblasts at the wound site, is believed to play an important role in wound contraction. Myofibroblasts share phenotypic characteristics of both fibroblast and smooth muscle cells, including expression of α-SMA. Studies performed in animals have shown that cutaneous wounds in fetuses heal by the reformation of normal tissue architecture without scar formation. Adzick et al. expanded on this research and developed a model to study human fetal skin wound healing. Human fetal skin grafts were placed into athymic (hairless, lacking normal thymus and immune system) mice. The full-thickness grafts were taken at various gestational ages implanted in two groups; one cutaneously and thereby exposed to air, and the other in a subcutaneous pocket below the panniculus carnosus. Linear incisions were made in the grafts 7 days after implantation. After varying time periods (7-21 days) the grafts were excised and analyzed histologically for scar formation. [4] Click image for schematic of procedure.
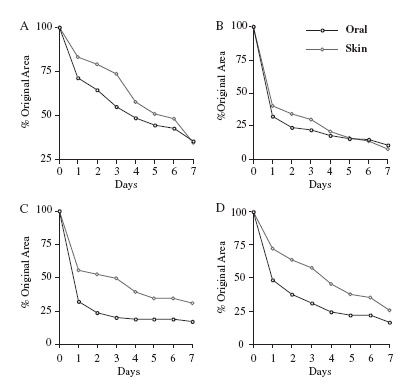
It was found that all incisions in the subcutaneously implanted grafts healed with no scar formation regardless of gestational age of the donor. In contrast the cutaneously implanted tissues experienced scar formation at the site of incision as well as the interface of adult mouse skin and the human fetal graft. Also, control grafts of both adult human and adult mouse tissue that were implanted subcutaneously experienced scarring. The results demonstrate that: (1) human fetal skin heals without scar formation in a subcutaneous adult environment; (2) scarless repair of fetal skin tissue does not depend on either perfusion by fetal serum or the unique amniotic fluid environment; (3) cutaneous grafts of fetal tissue heal with scar formation. [4] Adzick et al. suggested that the fetal fibroblast plays a central role in manipulating fetal wound healing. Wounds in the oral mucosa heal faster and with reduced scarring as compared with cutaneous wounds. Irwin et al. hypothesized that the differences in healing outcomes between the oral mucosa and skin could be due to phenotypic differences in their respective fibroblast populations. Their study compared mucosal and dermal fibroblasts in terms of collagen gel contraction, α-smooth muscle actin (α-SMA) expression, and production of the epithelial growth factors keratinocyte growth factor (KGF) and hepatocyte growth factor/scatter factor (HGF). Also studied was the effect of transforming growth factor-β (TGF-β) on the wound healing. [5] Click image for graph of wound sizes versus time.
Although the presence of myofibroblasts early in the wound healing process is beneficial in contracting of the wound and thereby reducing its size, the retention of myofibroblasts appears to increase the risk of scarring. This is interesting because other in vivo studies have shown that myofibroblasts are not found in early gestational wounds that heal without scarring, while they are present in later gestational wounds that heal by scarring. Irwin et al. suggest that reduced numbesr of myofibroblasts at oral mucosa wound sites (as supported by the decreased expression of α-SMA) may account for the reduction in scar tissue seen in oral wounds compared to dermal wounds. Also worth noting is that increased numbers of myofibroblasts have been reported in fibrotic conditions such as scleroderma, pulmonary fibrosis, and hepatic cirrhosis. [6] Further understanding of the factors controlling myofibroblast differentiation and subsequent disappearance from wound sites could lead to therapeutic strategies to reduce scar formation. TGF-β1 has been shown to induce fibrosis in fetal wounds [7] and increased TGF-β1 expression has been found in several adult fibrotic conditions. [6] Irwin et al. found that the level of collagen gel contraction and α-SMA expression co-correlated with TGF-β1 in a dose dependent manner. This is explained by the hypothesis that TGF-β1 stimulates fibroblast differentiation to myofibroblasts. Other studies have found that TGF-β1 is lower in oral wounds that cutaneous wounds. [2] Following the hypothesis, this would lead to fewer myofibroblasts and explain the reduced scarring in oral mucosa wound as compared to cutaneous wounds. |
Click Links to Navigate Site |
| Website by Nick Gunn | June 11 2007 | Created for BME 240 @ UCI |