| Introduction | Embryoscopy and Fetoscopy | Applications | Future Directions | References |
Embryofetoscopy
can be utilized to study embryonic development through direct visualization of
structures, anomalies and developmental milestones, especially those in aborted
embryos as risk of failure is not as catastrophic. For example, at 6 weeks fetal
face can show forehead, widely spaced eyes, oral and nasal cavities and by week
10 the facial features become more prominent.
Development of trunk and limbs, closure of the neural tube by week 9 as
well as fully developed hands and feet can also be seen [2]. The embryo itself is very difficult to
examine after it has been evacuated due to damage during surgery or spontaneous
vaginal exit. Employing embryofetoscopy
before evacuation occurred can thus allow to examine the embryo in its intact
condition and thus study developmental defects and causes for death in utero,
which can often originate from single gene defects or abnormal karyotypes. Obtaining this knowledge can further help the
parents avoid recurrence of the defects in future pregnancies [1].
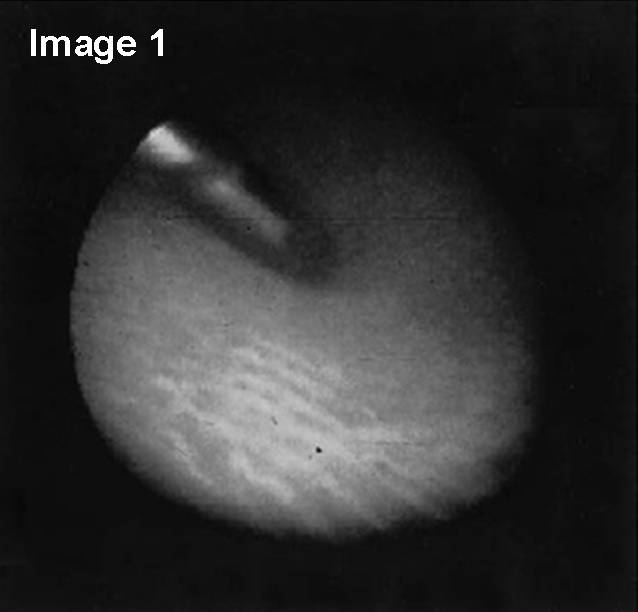
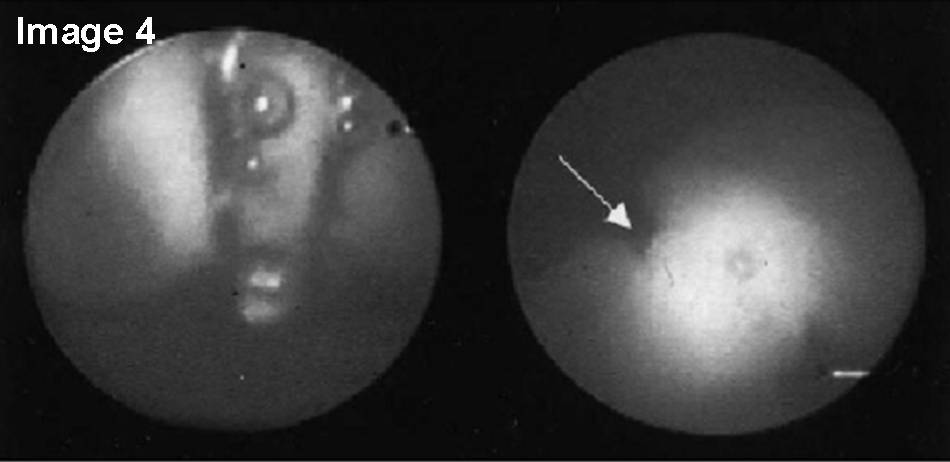
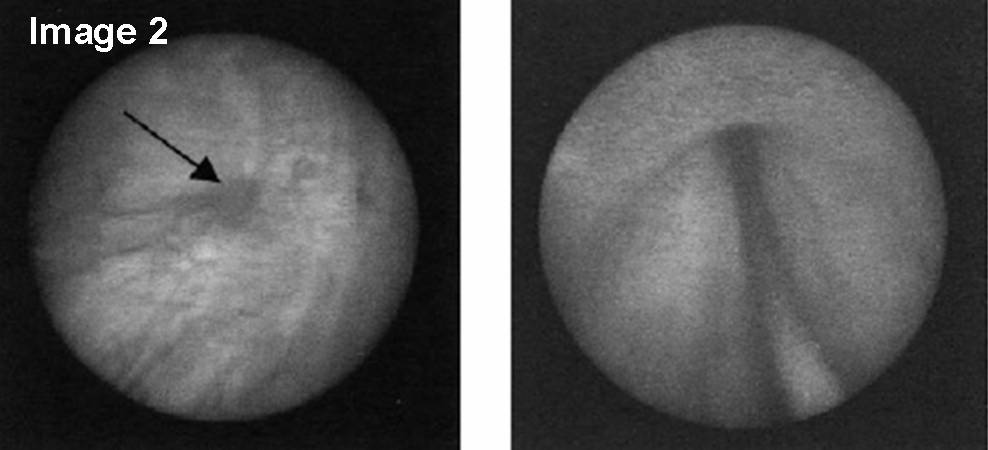
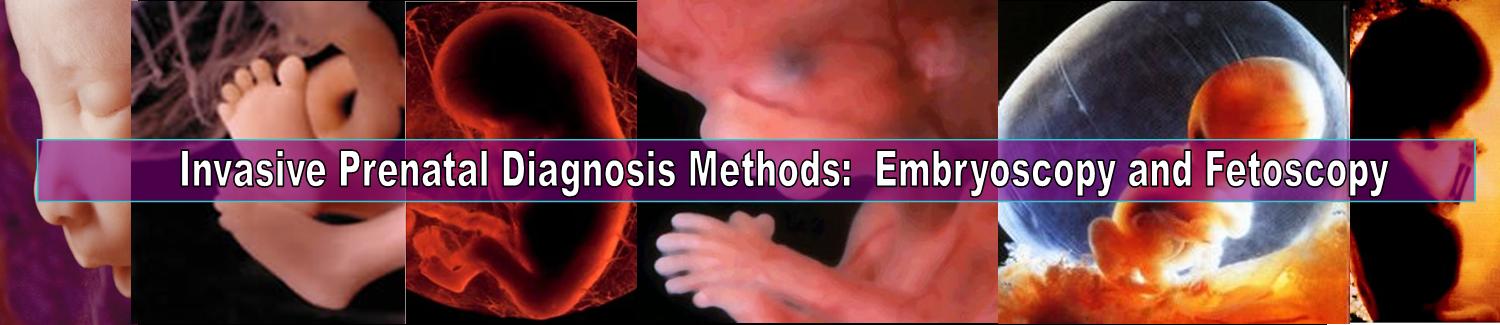
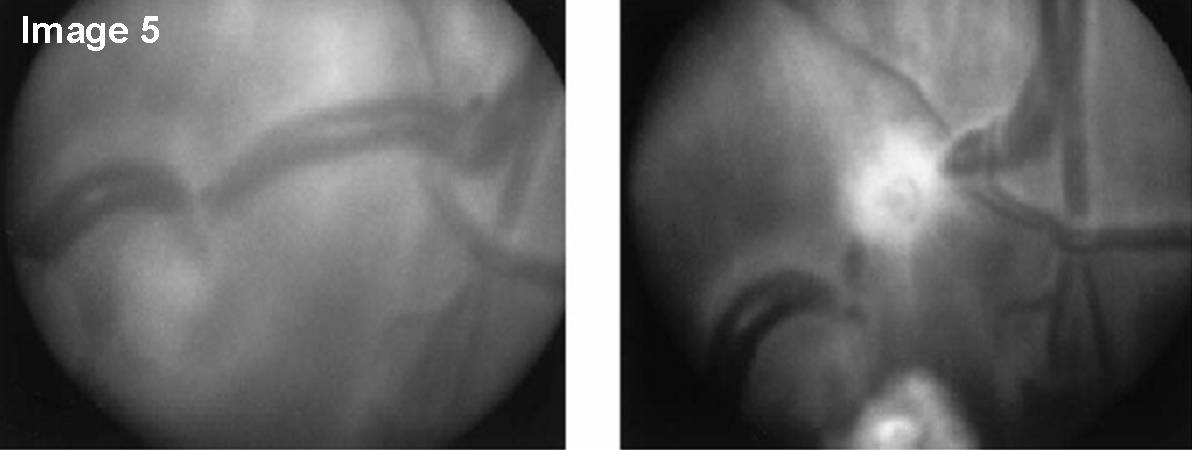 Figure 4: Image 1--Fetoscopic view of muscle biopsy being performed on a fetus at 18 weeks'gestation; Image 2--Fetal
antegrade cystourethoroscopy. (Left) Trabeculated bladder
but nondilated ureteral orifice (arrow). (Right) Wire
probe verifying presence of urethral atresia; Image 3--Fetoscopic view of a constricting amniotic band around the upper extremity of a fetus with amniotic band syndrom; Image 4--Fetoscopic
view of cord coagulation for TRAP sequence. (Left)
Umbilical cord being grasped by the bipolar device and
bubbles forming as heat is generated during cord coagulation.
(Right) Umbilical cord after coagulation (arrow); Image 5--Fetoscopic
view of chorioangiopagus on a monochroionic placenta before and after
selective fetoscopic laser photocoagulation in a case of severe TTTS.
(Left) An artery entering a cotyledon and a vein draining
the same cotyledon crossing to the opposite twin. (Right)
Blanched area of the photocoagulated vein.
Figure 4: Image 1--Fetoscopic view of muscle biopsy being performed on a fetus at 18 weeks'gestation; Image 2--Fetal
antegrade cystourethoroscopy. (Left) Trabeculated bladder
but nondilated ureteral orifice (arrow). (Right) Wire
probe verifying presence of urethral atresia; Image 3--Fetoscopic view of a constricting amniotic band around the upper extremity of a fetus with amniotic band syndrom; Image 4--Fetoscopic
view of cord coagulation for TRAP sequence. (Left)
Umbilical cord being grasped by the bipolar device and
bubbles forming as heat is generated during cord coagulation.
(Right) Umbilical cord after coagulation (arrow); Image 5--Fetoscopic
view of chorioangiopagus on a monochroionic placenta before and after
selective fetoscopic laser photocoagulation in a case of severe TTTS.
(Left) An artery entering a cotyledon and a vein draining
the same cotyledon crossing to the opposite twin. (Right)
Blanched area of the photocoagulated vein.Moreover,
embryofetoscopy can be theoretically used for fetal blood sampling and therapy
much earlier than currently existing technologies would allow. Not having to wait for the 2nd
trimester to obtain results about deviant chromosomes can significantly
decrease parents’ anxiety and allow the opportunity for early termination if
necessary. Some headway has already been
accomplished in this area when Reece et al. [8] obtained a small aliquot of
blood by using 3.5-mm fiber-optic endoscope passed transcervically [1].