 |
|
|
Home | Clinical Background and Need | Engineering Principles and Clinical Considerations | Commercial Devices | Upcoming Advancements |
| Engineering Principles and Clinical Considerations Proximal vs. Distal Engagement Given an access site proximal to the occlusion, the biggest consideration is whether to engage the thrombosis from the proximal or distal side. Proximal engagement techniques include vacuum only devices (catheter + vacuum source, such as a syringe), vacuum with thrombus penetration (like the Penumbra system), vacuum with rotary blade mechanism, or grabbing and pulling with no vacuum. Distal engagement techniques include helical coils (like the Merci Retriever) and cages for ensnaring the thrombus.
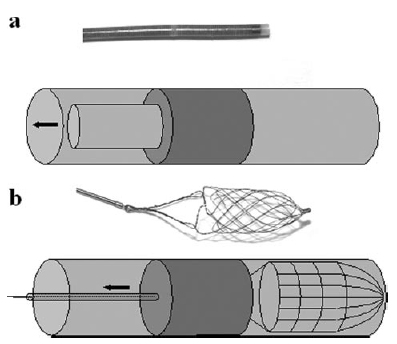
Figure 1. Vacuum only device (catheter + vacuum source), Balt Vasco35 (A). Cage for distal ensnaring of thrombosis, Balt Catch (B) (1).
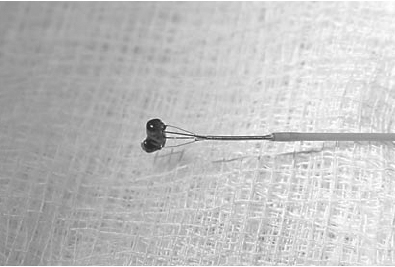
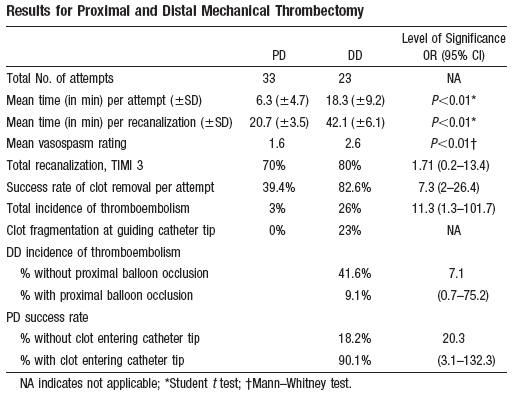
Figure 2. Grab and Pull; No Vacuum. Off-label use of the EV3 AlligatorTM Retrieval Device to Remove Middle Cerebral Artery Thrombosis (6) Compared to the distal approach, the proximal approach has a significantly shorter time per attempt at thrombus retrieval and overall recanalization time and a significantly lower vasospasm rating. However, the proximal approach has a significantly lower success rate of clot removal per attempt and a lower total recanalization rate compared to the distal approach. The proximal approach has a low incidence of thromboembolism, while the distal approach has an appreciable incidence of thromboembolism. However, utilizing a proximal balloon occlusion to occlude antegrade blood flow greatly reduces the incidence of thromboembolism in the distal approach; there is no effect of proximal balloon occlusion in the proximal approach (1). Refer to Figure 3 for greater detail. Time to recanalization is a very critical parameter because patient outcomes have been strongly tied to the amount of time with obstructed blood flow to the brain. Compared to distal engagement of the thrombosis, proximal engagement enables a shorter time to recanalization, but is less effective at achieving recanalization.
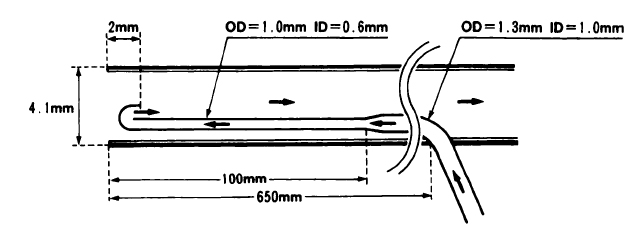
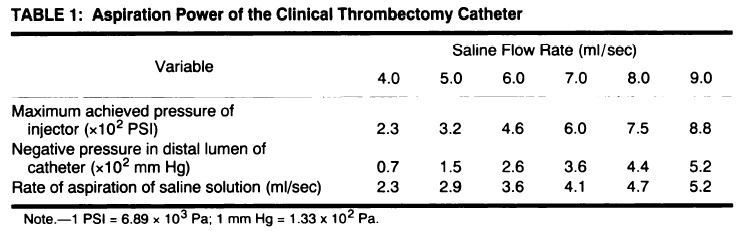
Figure 3. Results for Proximal and Distal Mechanical Thrombectomy in Swine (1). Method of Vacuum Devices employing proximal engagement of thrombosis, and even some distal engagement devices, utilize a vacuum during the procedure to retrieve the thrombosis. There are various ways to achieve vacuum. The most common and simplest methodology, aspiration with a syringe, has proven efficacy within an approved thrombectomy device (Merci retrieval system) as well as on its own. A simple configuration of a 20cc syringe attached to a 4.3F catheter has shown to be efficacious in recanalization (2). In addition, different sizes of syringes enable a choice in amount of vacuum to apply- greater vacuum is achieved by a greater stroke volume of the syringe. The downside is that the stroke volume of the syringe corresponds to the amount of blood withdrawn from the patient, so increasing the vacuum increases the amount of blood drawn from the patient. Another downside to the manual syringe aspiration technique is that there is no control of vacuum applied- the user can (inadvertently) change the vacuum applied by changing the stroke distance of the syringe’s plunger. Saline-jet aspiration catheters are composed of an inner and outer tube; the inner tube outer diameter (OD) is typically a fraction of the outer tube inner diameter (ID). The inner tube bends 180 degrees at the distal end to form a proximally-directed outflow. The outflow of the inner tube is typically located slightly proximal to the tip of the outer tube. Saline is controllably supplied to the inner tube via a reservoir tank/flow rate pump system. The flow rate of saline through the inner tube is thus easily controlled. Saline exits the outflow of the inner tube and flows in the proximal direction through the outer tube. This creates a negative pressure gradient at the distal end of the outer tube due to the Venturi effect (3). See Figure 4.
Figure 4. Inner catheter supplies a jet-stream of saline (direction of flow indicated by the arrows), creating a Venturi effect in the larger catheter (3)
Figure 5. Bernoulli Law Derivation (4) Given a pipe and a fluid flowing through it at a steady rate (see Figure 5, above), the work, W, done by applying a pressure P over an area (A), resulting in a linear offset (in axis of flow) and thus volume change of ΔV. Then the work, W, done by the pressure, P, is given by dW = P*dV At points 1 and 2 in the image above, this equates to ΔW1 = P1ΔV1 and ΔW2 = P2ΔV2 Therefore, ΔW1 - ΔW2 = P1ΔV1 - P2ΔV2 But work is a function of kinetic (K) and potential (U) energies: ΔW = ΔK + ΔU = Δ(1/2)mv2 + Δmgh where m = mass; v = velocity; g = gravitational constant; h = height Therefore, P1ΔV1 - P2ΔV2 = Δ(1/2)mv22 – Δ(1/2)mv12 + Δmgh2 – Δmgh1 Rearranging gives: P1 + (Δmv12)/(2ΔV) + (Δmgh1)/(ΔV) = P2 + (Δmv22)/(2ΔV) + (Δmgh2)/(ΔV) And using ρ = m/V, where ρ = density P1 + (1/2)ρv12 + ρgh1 = P2 + (1/2)ρv22 + ρgh2 This is referred to as the Bernoulli Law (4). Now dividing both sides by ρ and assuming that h1 = h2 P1/ρ + (1/2)v12 = P2/ρ + (1/2)v22 Replacing velocity with flow rate: v = (4Q)/(pi*D2) where Q = flow rate; D = diameter gives: (P1 - P2) = ΔP = ρ*(1/2)*[ (16)/(pi*D24) - (16)/(pi*D14) ]*Q2 (5)
(1) Gralla J, Schroth G, Remonda L, Nedeltchev K, Slotboom J, Brekenfeld C. Mechanical Thrombectomy for Acute Ischemic Stroke: Thrombus-Device Interaction, Efficiency, and Complications In Vivo. Stroke, 37: 3019-3024. 2006. (2) Jankowitz B T, Aleu A, Lin R, Jumaa M, Kanaan H, Kostov D, Hammer M, Uchino K, Wechsler L R, Horowitz M, Jovin T G. Endovascular Treatment of Basilar Artery Occlusion by Manual Aspiration Thrombectomy. J NeuroIntervent Surg, 2: 110-114. 2010. (3) Yamauchi T, Furui S, Irie T, Makita K, Takesita K, Katoh R, Kusano S. Saline-Jet Aspiration Thrombectomy Catheter. AJR, 161: 401-404. 1993. (4) Romero D. Bernoulli's Law. (5) Venturi Calculator. Flowmeter Directory. (6) Lee R, Lui W M, Cheung R T F, Leung G K K, Chan K H. Mechanical Thrombectomy in Acute Proximal Middle Cerebral Artery Thrombosis with the Alligator Retrieval Device. Cerebrovasc Dis, 23: 69-71. 2007. |
 (1)
(1)
 (3)
(3)