|
|
|
Home | Clinical Background and Need | Engineering Principles and Clinical Considerations | Commercial Devices | Upcoming Advancements |
|
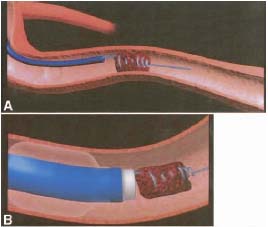
Commercial Devices in the United States (FDA Approved) Merci Mechanical Clot Retriever (Concentric Medical, Mountain View, California) Markets: 510k (US), CE Marque (Europe) How it Works: The system consists of a balloon guide catheter, a microcatheter, and the Merci Retriever. The access site is the femoral artery. The technique is summarized in Figure 1. First, the balloon guide catheter is advanced near the blockage location using standard angiographic techniques (via guidewire). It is placed in the internal carotid artery for anterior vasculature access or the subclavian artery for posterior vasculature access. Then the microcatheter is advanced through the balloon guide catheter, and the microcatheter and guidewire are advanced through and beyond (distal to) the blockage. To minimize the risk of distal embolism, the microcatheter and guidewire are passed between the vessel wall and the thrombosis with great care such that they do not contact the thrombosis. The guidewire is then retrieved, and the Merci Retriever is advanced through the microcatheter. The Retriever is made from a platinum memory-wire with a pre-shaped, five-loop tapered helix. This construction allows the Retriever to be advanced through the microcatheter in a linear form but be deployed in the vessel in its coiled formation. Deployment consists of advancing the Retriever out of the microcatheter, with the microcatheter located distal to the blockage. The vessel length distal to the blockage must be at least 2 mm to accommodate the loops of the Retriever. The Retriever and microcatheter are retracted to engage the thrombosis with the distal loops of the Retriever. The microcatheter is then further retracted and the Retriever is torqued clockwise (maximum five revolutions) to engage the thrombosis with the proximal loops of the Retriever and thus fully ensnare the thrombosis (see Figure 2, part A). The microcatheter is then advanced to the proximal end of the thrombosis (approximately 2 mm behind the most proximal loop of the Retriever). The balloon (from the balloon guide catheter), located either in the internal carotid artery or the subclavian artery, is then inflated to occlude antegrade blood flow. Aspiration, and thus vacuum suction, is applied through the lumen of the balloon guide catheter with a 20 mL syringe while the microcatheter and Retriever are simultaneously retracted through the balloon guide catheter (see figure 2, part B). If significant resistance is met due to stenosis or tortuous anatomy, the Retriever can be rotated counter-clockwise (two to three revolutions only) to reduce its profile and device tension. More vigorous aspiration (a stronger vacuum) is then applied when the thrombosis is at the tip of the balloon guide catheter to pull the thrombosis into the balloon guide catheter (1), (2).
Figure 1. Summary of Merci System Technique (2)
Figure 2. A. Thrombosis is fully ensnared by Retriever. B. Retriever, microcatheter, and thrombosis are retracted through the balloon guide catheter while the balloon is inflated and aspiration is applied. (1)
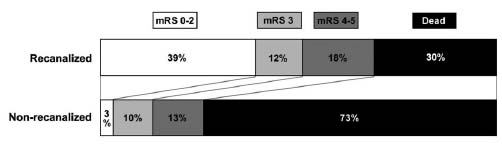
Clinical Results: 80 patients total (MERCI and multi MERCI Part I trials) Main Exclusion criteria: -- Time of presentation was greater than 8 hours from symptom onset -- National Institute of Health Stroke Scale score was less than 8 -- Cerebral hemorrhage seen in CT scan (3) Spontaneous recanalization rate in acute stroke is estimated around 17-18% from data from other trials. Recanalization rate using intravenous t-PA was 26% (data from another trial). The MERCI and multi MERCI trials did not have a nontreatment arm and thus cannot claim that mechanical thrombectomy is superior to nontreatment. However, the data does support that 53% had successful recanalization with the Merci Retriever alone, and 63% had recanalization with the Merci Retriever and adjunctive endovascular treatment. Recanalization is associated with better clinical outcome and survival as shown in Figure 3 (4).
Figure 3. Patient outcome according to recanalization status. Lower modified Rankin Score (mRS) corresponds to better patient outcome (4).
Merci Retriever: X6-Series: Non-filamented Retriever. Able to be resheathed in vivo. Evaluated in the MERCI trial. L-Series: Second generation, filamented Retriever. Filaments provide increased surface area for thrombosis removal. Not able to be resheathed in vivo. Evaluated in the Multi-MERCI trial. V-Series: Third generation, filamented Retriever. Variable pitch enables proximal loops to stretch while distal loops remain intact (see Figure 4). Not able to be resheathed in vivo. Information and images for X6, L, and V Series Retrievers were obtained from (2).
Figure 4. V-Series' variable pitch enables proximal loops to stretch while distal loops remain intact (2).
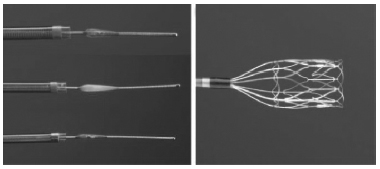
Penumbra SystemTM (Penumbra, Inc., Alameda, California) Markets: 510k (US): Penumbra System only CE Marque (Europe): Penumbra System and Direct Thrombus Extraction How it works: The system consists of a reperfusion catheter, a SeparatorTM, and an aspiration pump (and a thrombus removal ring and balloon guide cather, Europe only). The access site is the femoral artery. First, the reperfusion catheter is advanced to the proximal side of the blockage location using standard angiographic techniques (via guidewire). The guidewire is then retracted, and the Separator is advanced through the perfusion catheter. The aspiration pump is then turned on to maintain a constant aspiration vacuum of -20 in Hg throughout the procedure. The Separator is advanced beyond the tip of the perfusion catheter to engage and penetrate the thrombosis. The Separator is repeatedly retracted (completely) and advanced (distal portion fully deployed in vivo) through the reperfusion catheter into the proximal end of the thrombosis to break up the thrombosis, while the aspiration sucks the fragments of the thrombosis through the reperfusion catheter. The reperfusion catheter is advanced as needed throughout the procedure to maintain its engagement to the thrombosis. (5) If the thrombosis is unable to be extracted, direct extraction via a thrombus removal ring is performed. A balloon guide catheter is advanced proximal to the blockage location using standard angiographic techniques (via guidewire). The reperfusion catheter is then advanced through the balloon guide catheter and positioned approximately 15 mm distal to the occlusion location. A thrombus removal ring, sized appropriately based on vessel diameter, is then advanced through the reperfusion catheter in a crimped configuration. The aspiration pump is then turned on to maintain a constant aspiration vacuum of -20 in Hg during the procedure. The ring is then deployed from the reperfusion catheter and the catheter and ring are advanced together until the tip of the catheter is embedded into the thrombosis and the ring is embedded at least 1 cm into the thrombosis. The balloon is then inflated to occlude antegrade blood flow. The thrombus removal ring and reperfusion catheter are then retracted through the balloon guide catheter. Finally, a syringe is used to aspirate approximately 10 mL of blood through the balloon guide catheter to remove any residual thrombosis fragments remaining after the retraction of the thrombus removal ring and reperfusion catheter (6).
Figure 5. Penumbra repurfusion catheter and Separator (left); thrombus removal ring (right) (6).
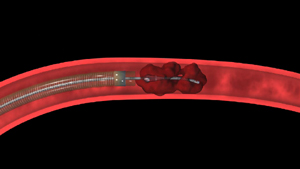
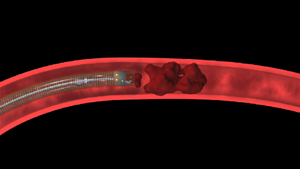
Figure 6. Separator is placed into the thrombosis with the reperfusion catheter engaging the thrombosis (left). Separator is retracted into the reperfusion catheter (middle). Separator is repeatedly retracted and advanced into the thrombosis, and the reperfusion catheter is advanced to maintain its engagement to the thrombosis (right) (5).
Clinical Results: 125 patients Main exclusion criteria: -- Time of presentation was greater than 8 hours from symptom onset -- National Institute of Health Stroke Scale score was less than 8
-- Thrombolysis In Myocardial Infarction Grade greater
than 1
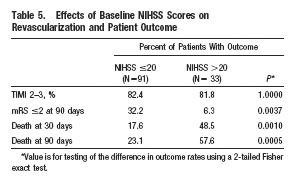
81.6% of the treated patients were successfully revascularized to Thrombolysis In Myocardial Infarction Grade 2 to 3. Despite 28% of patients having intracranial hemorrhage and 32.8% all-cause mortality at 90 days, the Penumbra System was deemed safe and effective to revascularize patients experiencing ischemic stroke who presented within 8 hours of symptom onset (6). Table at the right from (6).
(1) Martinez H, Zoarski G H, Obuchowski A M, Stallmayer M J B, Papangelou A, Airan-Javia S. Mechanical Thrombectomy of the Internal Carotid Artery and Middle Cerebral Arteries for Acute Stroke by Using the Retriever Device. Am J Neuroradiol 25: 1812-1815. 2004. (2) Concentric Medical: Merci Retriever System (3) Mechanical Embolectomy for Treatment of Acute Stroke. Anthem Medical Policy # SURG.00098. 2010. (4) Flint A C, Duckwiler G R, Budzik R F, Liebeskind D S, Smith W S. Mechanical Thrombectomy of Intracranial Internal Carotid Occlusion: Pooled Results of the MERCI and Multi MERCI Part I Trials. Stroke 38: 1274-1280. 2007. (5) Penumbra Inc: Penumbra System (6) The Penumbra Pivotal Stroke Trial Investigators. The Penumbra Pivotal Stroke Trial. Safety and Effectiveness of a New Generation of Mechanical Devices for Clot Removal in Intracranial Large Vessel Occlusive Disease. Stroke, 40: 2761-2768. 2009. |