Femtosecond Laser Glaucoma Treatment:
The femtosecond laser has emerged in recent years with a warm reception from the biomedical community. The reason for this is that pulse durations on the order of femtoseconds can be targeted very specifically within biological tissue. The reason for this is the incredibly short pulse duration. It essentially prevents collateral damage caused by non specific heating of surrounding tissues. This is one of the drawbacks concerning argon laser trabeculoplasty. As result, scarring is minimized greatly while efficacy is still maintained.
A current approach is the titanium sapphire femtosecond laser system. These systems can be tuned to deliver wavelengths between 775 and 1700 nm with pulse durations lasting less than 100 fs at the end of the optical path. It should be noted now that the method of action is no longer heating and scarring but rather photo-disruption of the biological tissue. The wavelengths chosen are to be optimized by avoiding wavelengths with strong absorption in water. The reason for this is that the femtosecond technique is fundamentally different in approach from trabeculoplasty. As mentioned before, the physical mechanism of action is not heating and burning but rather photodisruption.
Photodisruption occurs when laser power intensity is large enough to induce optical breakdown in a material: the laser pulse transforms the material into plasma. The strong optical intensities required for photodisruption can be achieved at the focus of a high peak power laser beam. Breakdown occurs only where the intensity is larger than the threshold level. Below this threshold level, the laser pulse passes through the material without causing damage. Thus, the location of optical breakdown can be controlled to occur only at the focus of the beam where the intensity exceeds the threshold level. If the laser is focused beneath the surface of a material, subsurface breakdown occurs only at the focus. No damage occurs in the material that the beam was focused through [5].
This is why the femtosecond laser differs so much from the traditional argon trabeculoplasty. The only point of photodisruption will be at the focus of the laser. And depending on the wavelength chosen the focus can be moved well below the surface of the tissue. This is in direct contrast to the argon laser treatment where the laser heats tissue in a very nonspecific collateral way.
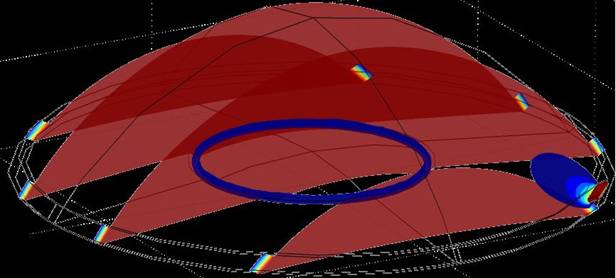
As result, the femtosecond titanium sapphire laser can create very well defined channels beginning in the trabecular meshwork, passing through the schlemm’s canal, and ending within the sclera. The advantage of this approach is that it gives the AH in the anterior chamber a direct route to the schlemm’s canal and collector channels. Since photodisruption is very specific there is minimal scarring. In addition, a few small channels should be more than enough to increase the outflow facility to therapeutic levels. The following image is a computer generated model predicting the effect of one such channel.
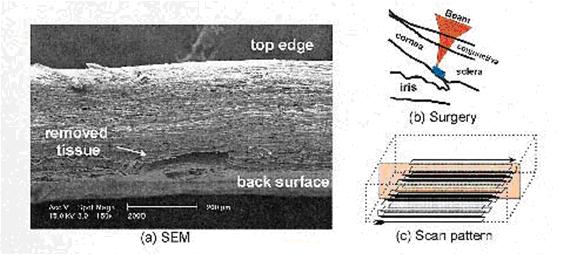
A study at the University of Chicago in 2005 showed the feasibility of the Ti:Sapphire femtosecond laser in photodisrupting the human trabecular meshwork without collateral damage [6]. This group used 75 fs pulses at two different pulse energies to demonstrate this end. In the micrographs it is obvious that collateral damage is minimal if not absent as very fine structures such as aqueous veins and the border of schlemm’s canal are preserved.
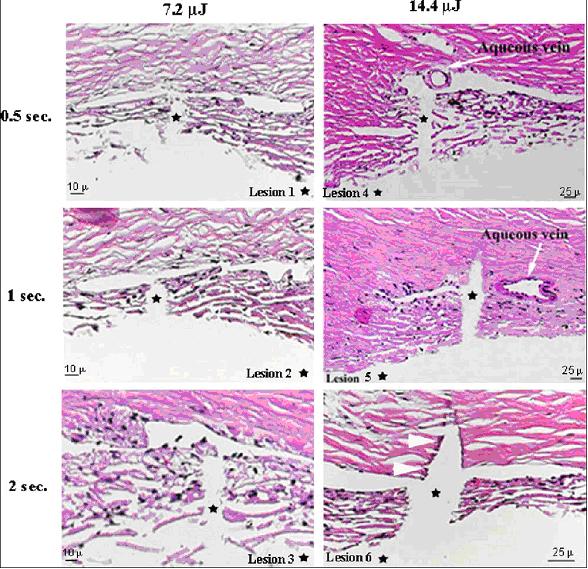
“ Fig. 2. Microphotographs showing histology of fsec LTA lesions in the human trabecular meshwork. Average dimensions of the lesions are given in Table 1 .
Lesions 1, 2, and 3: fsec LTA at a pulse energy of 7 $ 2 m J at varying durations (0 $ 5, 1, and 2 sec, respectively). Note the sharp margin of the lesions through the
TM and into Schlemm’s canal and preservation of the outer wall of the canal. Lesions 4, 5, and 6: fsec LTA lesions at a pulse energy of 14 $ 4 m J at varying
durations (0 $ 5, 1, and 2 sec, respectively). Note the size and collateral damage of the lesion with the higher dose (arrowheads). (H&E; original magnification,
20 ! ). ”
Wavelength Selection:
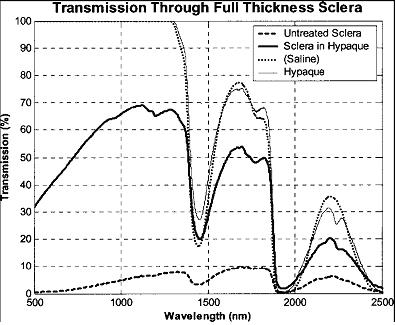
The wavelength is a crucial parameter in determining the success of femtosecond laser glaucoma treatment. As mentioned before, one must avoid wavelengths with absorption peaks in water. This is obvious as living tissues are composed primarily of water. In relation to creating a subscleral surgical channels aimed at reducing IOP, a wavelength must be chosen that not only has low absorption in water, but high transmission in scleral tissue. The sclera is a very optically scattering tissue which poses a problem especially since the technology hinges on being able to produce a tight laser focus beneath the surface of the tissue. Water has strong absorption at 1450 nm and 1900 nm while scleral tissue is relatively transparent at 775 nm and 1060 nm [5]. Thus, one can choose a wavelength for optimal efficacy.