| Introduction | Embryoscopy and Fetoscopy | Applications | Future Directions | References |
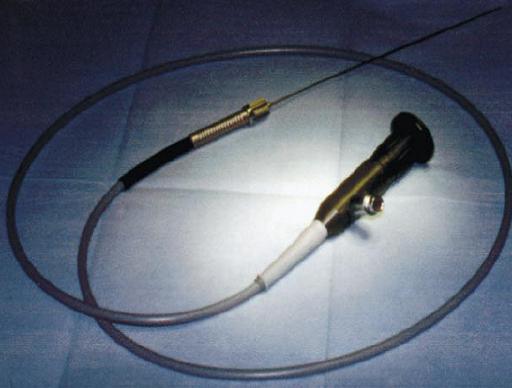
Embryoscopy and fetoscopy are sometimes referred to as embryofetoscopy. Embryofetoscopy is capable of providing knowledge about embryonic development as well as provide a method for prenatal investigation of high-risk pregnancies for recurrent genetic disorders, perform fetal intravascular transfusions, and allow access to the embryo circulation [1,2]. Embryoscopy refers to visualization of the embryo 5 to 8 weeks after conception, while fetoscopy deals with visualization of the fetus 8 weeks following gestation. Both procedures are performed via insertion of a high-resolution fiber-optic scope transadbominally or transcervically, either into the extracelomic space (before 11 weeks after conception) thus allowing visualization of the embryo through an intact amnion membrane, or into the amniotic cavity (after 11 weeks) [1]. A typical endoscope can vary from 1.7mm to 3.5mm in diameter and 0 to 30° in lens angle and is passed using ultrasound guidance [1]. Zero degree endoscopes are also used with resolution up to 50,000 pixels [3] (Figure 1).
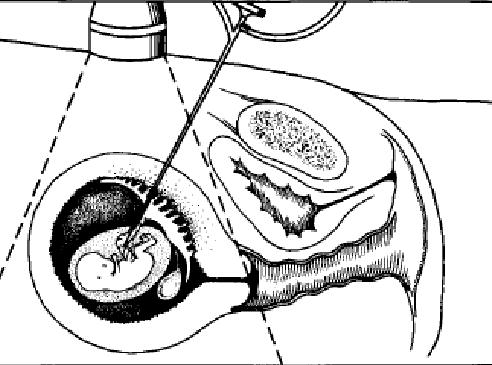
Figure 2: Schematic
diagram of an embryoscope inserted transcervically
and passed
through the chorion into extraoelomic space [2]
Figure 1: Embryoscope [3]
Once the
scope reaches the opaque chorion, a rapid blunt thrust by the tip of the
endoscope has to be applied perpendicular to the chorionic membrane to allow
penetration into the extracoelomic space (Figure 2) [2]. This procedure has to be performed very
carefully to avoid areas of amnion and chorion juxtaposition as well as
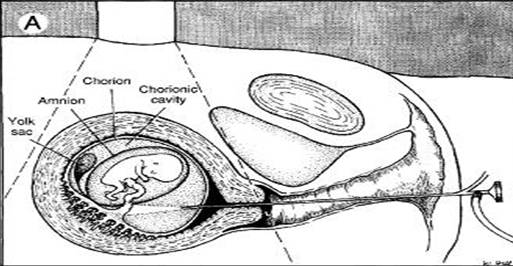
the placenta [2]. Consequently, phenotypical
properties of the fetus such as head, face, dorsal and ventral walls, umbilical
cord and yolk sac can be observed. Video
recording through the scope can also be done for more thorough examination at a
later date.