ECoG surgery techniques were first used by Penfield and Jasper in the 1950s to map focal inter-ictal spiking and determine the extent of resection (1). Thus, for the last six decades, ECoG surgery as been used to localize epileptogenic zones, map cortical functions, and predict the success of the resection surgery.
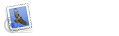
In order to use ECoG electrodes to localize epileptogenic zones, there are many layers of tissue that covers the cerebral cortex, or the outer portion of the brain that consists of layers of nerve cells and pathways that connect them. Also, the cerebral cortex is known as the part of the brain in which thought processes take place. Thus, there are two types of electrode placement on the cerebral cortex for recording neural activity; epidural or subdural placement. Epidural placement of electrodes is when the electrodes are placed on the outside of the dura matter (i.e. EEG placement), where subdural placement is underneath the dura matter (i.e. ECoG placement) (2). Figure 1 below shows the various tissue layers that lead to the cerebral cortex, and the location of the dura matter (i.e. the outermost, toughest, and most fibrous of the three meninges that cover the brain), where electrodes can be placed above or below this layer.

Figure 1: Tissue Layers of the Cerebral Cortex
Currently, ECoG is considered to be the “gold standard” for assessing neuronal activity in patients with epilepsy who have intractable epilepsy and must undergo surgical resection of a lesion on an epileptogenic zone (or an abnormal place in the brain where a seizure starts). Since the patient has already undergone an MRI scan and EEG recordings to assess the use of surgery, an ECoG array can then be implanted into the patient to determine the precise epileptogenic zone and lesion location. This is done by placing electrodes directly on the exposed surface of the brain to record electrical activity from the epileptogenic region in question determined from the MRI and EEG studies. Figure 2 below shows the surgical implant of an ECoG array on the cerebral cortex for epileptic zone localization. Note that this is for an extraoperative ECoG surgery, where ECoG is performed on a patient during a session not involving the removal of epileptogenic tissue (3). Intraoperative ECoG surgery is when the procedure is performed during a resection surgery of the epileptogenic zone.

Figure 2: Electrode Placement for Subdural ECoG on the Cerebral Cortex (3)
Unlike electroencephalography (EEG) techniques used prior to the ECoG surgery, EEG recordings cannot define the epileptogenic zone with the amount of sensitivity and defined boundaries that correct ECoG techniques can offer. Thus, in order to properly perform a resection surgery on the patient, the surgeon needs to define and remove/disconnect the region of the cortex that generates epileptic seizures without causing too many neurological or cognitive deficits (4). This is one of the many advantages for using ECoG extraoperative surgery to define epileptogenic zones for resection surgery. The following background will look further into the use of ECoG techniques for resection surgery to treat intractable epilepsy and who could benefit from this type of epilepsy surgery.