CHALLENGES

CHALLENGES
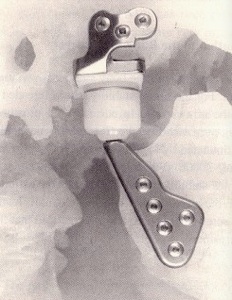
Any new artificial joint replacement should meet a lot of basic rules including biocompatibility, functionality, and safety. Specific requirements for TMJ prostheses were derived from the literature on TMJ replacements 1995(van Loon et al.). In the very beginning of TMJ replacement, people located the axle of the jaw rotation in the middle of the condyle head which limited the sliding movements of the prosthetic joint. (Fig. 1) When unilaterally applied, an incorrectly functioning TMJ prosthesis may cause dysfunction of the non-replaced contralateral TMJ. Then came the second kind of artificial TMJ imitated the forward sliding movement by the concept of an “inferiorly located” center of rotation. The center of rotation (CR) is located below the middle of the mandibular condyle. Using mathematical model, scientists simulated the three-dimensional mandibular movements and found that 15 mm inferior to the middle of the condyle is the “optimal” position for CR which best reduced the loss of forward sliding movements and also allow some sideward movements. (Fig. 2,3)
This is probably why using the second kind of artificial joint the load on the prosthetic side increases a great deal during molar bites. As the left and right sides must work at the same time to move the jaw, the incorrect imitation of the moving curve of the prosthetic TMJ will not only cause high wear rate of the spherical head but also diseases or dysfunction of the contralateral nature joint. So a proper stretchable set, for example, a spring must be add to either the mandibular side or the skull side of the joint to make the imitation of the biting curve possible.
The second noticeable problem is that while studying the stresses in the joint and the strength of the material, the experiments only considered the opening and closing phases in the biting movements. That resulted in an expected total wear rate of 0.65 mm3 per year, corresponding to a total yearly decrease of disk thickness of less than 0.01 mm. It seems that these values are considered sufficient low enough to achieving a long lifetime. However, the chewing cycle can actually be divided into three phases: (a) the opening phase, the closing phase and the occlusal phase. What will happen during the occlusal (stroke) move, especially chewing some hard food? Another contradictory location is when the month is wide open, for example, when people are yawning or laughing heavily. These are the situations when the condyle has extreme displacements. If in these cases, the stress on the condyle is greatly larger than in regular move, the former artificial TMJ mentioned about might not fit the low wear rate requirements.
Another thing worth considering is the missing of the opening end point using a spherical head on the mandibular part (Fig. 2). During the mouth opening, the closing end point of the jaw movement is controlled by teeth occlusion, while lateral and forward movements of the jaw are controlled by the shape of the bones and the action of muscles and ligaments. Lacking normal force from muscles to the artificial disk, the jaw might move forward too much or cause above standard loads on the contralateral TMJ.


People used a three dimensional mathematical model to study the influence of the implantation on the non-replaced TMJ as well as on the prosthesis itself. However, it was found that the load on the natural contralateral TMJ remains within normal limits, while the load on the prosthesis side increases approximately 50%. The maximum load on the prosthetic side occurs during molar bites and is approximately 100N. Ultimately, molecular weight polyethylene (UHMWPE) was selected to make the disk and zirconium oxide ceramic was chosen for the skull part and the head of the mandibular part. Although, through preclinical wear tests, the wear rates of these materials are considered sufficiently low for achieving a long lifetime, problems still exist.
Considering the “low CR” model in Fig. 3, during the chewing, the condyle head move ahead and back having exactly the same trail. So does the jaw as a whole. But, it’s totally different in natural TMJ. This can be proven by the model proposed byB. Villamil etc. representing and simulating the temporomandibular joint that addresses specifically mandible movements involved in the mastication cycle. (Fig. 4) But Fig. 4 only shows the standard curve of the jaw movement through mastication cycle, in fact, the movement changes according to individual characteristics, including dental occlusion and number of teeth, as well as is affected by food type and size. (Fig. 5) Personal and circumstantial differences in the mastication cycle have been studied by several researchers in the last few years7-8. In these studies, experiments were made tracking the different patterns of jaw movement, especially those concerning to chewing foods with different textures.


Fig.1
Fig.2
Fig.3
Fig. 4
Fig. 5