Diagnostic Applications of TMS
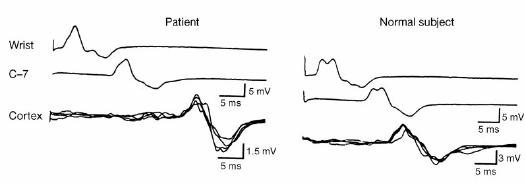
The primary diagnostic clinical function of TMS is to measure activity of neuronal circuits. The most frequently used is measuring the connection between the primary motor cortex and a muscle (i.e. MEP amplitude, MEP latency, central motor conduction time). This is most useful in stroke, spinal cord injury, multiple sclerosis and motor neuron disease. WIth TMS, it is possible to study the speed of conduction in central motor pathways. This method has been applied to evaluate patients with multiple sclerosis, which interfers with action potential conduction down the corticospinal tract. Measuring conduction time is a useful nonspecific diagnostic technique because slowing of conduction speed is commonly seen in neurodegenerative diseases. This method can also be used to diagnose cervical spondylosis, where very small motor disturbances must be detected. Figure 8 below compares motor conduction to the abductor digiti minimi muscle between a normal patient and a patient with extradural spinal cord compression, where stimulation is applied at the wrist, C-7 level of the spinal cord, and the cortex.
Figure 8
From these recordings, it can be seen that latencies are similar following stimulations at the wrist and spine, but the latency is much longer following cortex stimulation in the patient, which implies a longer central motor conduction time. [1]
Various parameters in the motor cortex can be measured by TMS. This allows us to evaluate different aspects of cortical excitability. The activity of interneurons in the cortex can be measured with intracortical inhibition (ICI) and facilitation (ICF). In these studies, an initial conditioning stimulus is given that is large enough to activate cortical neurons but small enough that no descending influence on the spinal cord can be detected. A second test stimulus, at suprathreshold level, follows after a short time. Intracortical influences initiated by the conditioning stimulus modulate the amplitude of the MEP produced by the test stimulus. At very short intervals, less than 5 ms, the MEP is inhibited, and at intervals between 8 and 30 ms it is facilitated. ICI is may be largely mediated by neurons containing gamma-aminobutyric acid (GABA). The silent period is a pause in ongoing voluntary electromyogram activity produced by TMS. Although the first part of the silent period is due in part to spinal cord refractoriness, the latter part is entirely due to cortical inhibition. ICI seen with paired pulse stimulation and the silent period reflect different aspects of cortical inhibition. [2]
Lastly, it is possible to measure the plasticity of the brain using rTMS. Abnormality of plasticity may correlate with abnormalities in other neurological conditions.
[1] Brunholzl, C. & Claus, D. Central motor conduction time to upper and lower limbs in cervical cord lesions. Arch. Neurol. 51, 245–249 (1994).
[2] Ziemann, U., Rothwell, J. C. & Ridding, M. C. Interaction between intracortical inhibition and facilitation in human motor cortex. J. Physiol. (Lond.) 496, 873–881 (1996).
[3] Mark Hallett. Transcranial magnetic stimulation and the human brain. Nature. Vol. 406, July 13, 2000.