This section discusses the design of one electromagnetic partially-implantable middle ear implant currently available on the market -- MED-EL's Vibrant Soundbridge.
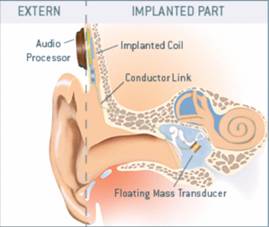
Symphonix’s Vibrant Soundbridge, shown above, consists of an external and an internal component. The external part, called the Audio Processor (AP), is worn on the head underneath the hair and held with a magnet and the internal part, called the Vibrating Ossicular Prosthesis (VORP), is implanted under the skin.

The AP (shown above), available in different colors to match hair color, consists of a microphone, digital signal processor (DSP), external coil, programming socket and battery compartment. The microphone picks up environmental sound, and the DSP processes the signal, by first dividing the input into several frequency bands and applying amplification algorithms such as linear amplification or wide dynamic range compression on individual bands to suit the individual's audiological profile. The output of all bands are summed and translated for mechanical vibration. The signal is then converted into RF energy for transcutaneous transmission through the external coil. The battery compartment holds a conventional type-675 hearing aid battery, which lasts approximately one week with normal use. The programming socket allows the audiologist to program the device according the patient’s hearing loss.
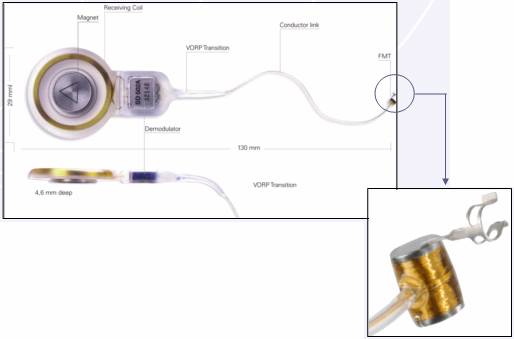
The VORP (shown above) consists of a magnet, receiving coil, demodulator, conductor link, and floating mass transducer (FMT). The magnet allows the AP to be held in position over the implanted part. The receiving coil is coupled with the external coil and the electromagnetic signal is demodulated and sent to the FMT via the conductor link. The FMT, attached to the incus, converts electric signal into vibrational energy, which are then transmitted to the inner ear via the ossicular chain.
The components of a partially-implantable middle ear implant, such as the external microphone, external audio processor, transmitting and receiving coils, modulation and demodulation circuitry, and data packet design, can be adopted from cochlear implant technology. Reviews on these topics can be found in literature and the design of such components can be found in the patent database. The only difference is in the actuator -- the cochlear implant uses an electrode array to stimulate different places along the cochlea whereas the middle ear implant uses an actuator (the FMT) that directly drives the middle ear ossicles.
The FMT has a "floating mass", which vibrates in response to a signal corresponding to sound waves. Electrical signals are sent to two electromagnetic coils wound around a hermetically sealed titanium housing. A magnet inside the housing supported by a pair of springs vibrates in response to the magnetic field generated by the electromagnetic coils, causing the entire structure to vibrate.
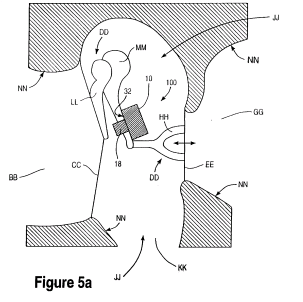
The floating mass is mechanically coupled to a housing, which is directly mounted on one of the middle ear bones, which is the incus in this case. The device's operation is based on the principle of conservation of energy, which states that energy can neither be created nor destroyed, but can only be changed from one form to another. Specifically, in a connected system of bodies, mechanaical energy is conserved (excludidng friction), and if one body loses energy, a connected body gains energy. (Ball et al, 1999)
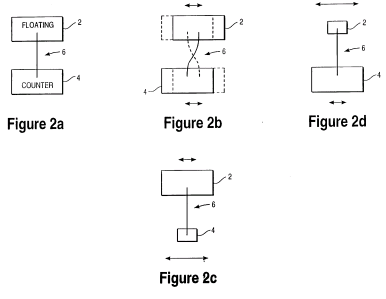
The figure below illustrates the basic theory of operation. Figure a below shows a floating block (FMT) connected to a counter block (incus) by a flexible connection. As the floating block vibrates in response to sound waves, mechanical coupling provided by the flexible connection allows vibrations to be transmitted to the counter block, which generally vibrates "counter" to the floating block. Figure b illustrates the "counter" vibration with arrows showing relative vibration of each block. The relative vibration of each block is inversely proportional to its inertia, which depends on mass and other factors (e.g. whether the block is connected to anoother structure). Figure b illustrates the case in which the relative inertia of two blocks are equal; in figure c, the mass of the floating block is greater than the counter block; and in figure d, vice versa. Case c is used when the FMT is designed to transduce mechanical vibration of the eardrum into electrical signals (e.g. as a sensor in a fully-implantable system (not yet available on the market) where the eardrum acts as a microphone); greater vibration of the counter block is desired for greater sensitivity. Case d is used in the Vibrant Soundbridge, where the FMT as an actuator transforms vibration into vibration of the incus. Having a floating mass with greater inertia also provides greater sensitivity.
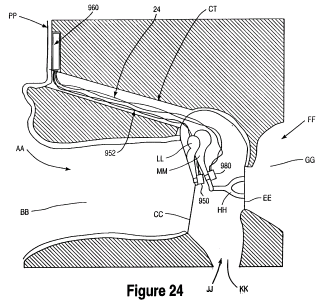
The FMT can be mounted on any vibrational structure in the ear with a mounting mechanism such as glue, adhesive, screws, clip, etc. The figure a below shows the FMT attached to the incus by a clip, and figure b shows a perspective view of the FMT.
The FMT is designed to mimic the vibratory response of the middle ear, and is capable of delivering mechanical stimulation with a frequency range corresponding to the speech frequency range. Laser doppler anemometry has been used to verify the device's operation. Clinical studies show that the device is safe and effective, and patients could hear as well with the device as conventional hearing aids. Changes in residual hearing are clinically insignificant. There is also significant improvements across various listening modes for the majority of patients, and qualitative reports from patients demonstrate a positive reaction.
|