

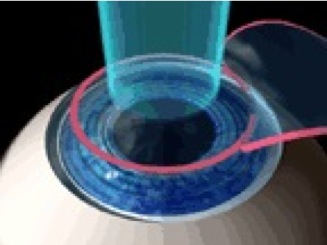
LASIK, laser assisted in situ keratomileusis, is classified as refractive surgery. A qualified ophthalmologists uses laser ablation to remove corneal tissue to correct for myopia, hyperopia, and astigmatism. Standard LASIK eye surgery requires that the surgeon cuts a LASIK flap with either a mechanical microkeratome or a femtosecond laser keratome. The flap thickness should be less than one third of the corneal thickness. After opening the flap, the laser ablates the underlying stromal tissue, based on the refractive correction needed. For myopic LASIK, the stroma tissue is removed from the cornea over the center of the pupil, thus flattening the cornea and reducing the refractive power of the eye. Hyperopic LASIK targets the cornea over the periphery of the pupil, increasing the corneal curvature and adding power to the cornea.
{kind=link}
The ablation profiles of excimer lasers have been developed over the last 20 years. The traditional LASIK profile, Munnerlyn’s formula, was used to correct for myopia and myopic astigmatism. Based on subjective and objective measurements of refraction, the laser is programmed to remove a convex-concave shape of corneal tissue.
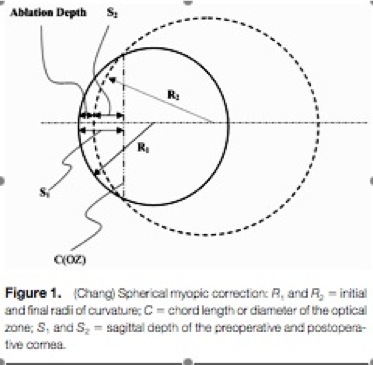
R1 and R2 are the initial and final corneal curvatures respectively. C is defined as the chord length of the optical zone (OZ), and S1 and S2 are the sagittal depths of the preoperative and postoperative cornea.
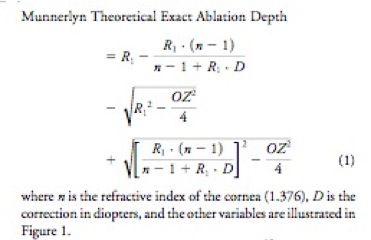
The approximate ablation depth used clinically based on Munnerlyn’s formula is removing 11 microns for every 1 diopter of refractive correction.
The latest LASIK excimer lasers have moved beyond Munnerlyn’s ablation profile. In order to reduce the complications of LASIK (i.e. glare, halos, etc.), four other ablation profiles are on being developed for commercial use.
Wavefront-Guided LASIK - uses a wavefront sensor to measure and approximate the wavefront of the eye, fitting to either Zernike polynomials or Fourier analysis. The profile is calculated based on the wavefront to minimize corneal aberrations.
Wavefront-Optimized LASIK - maintains the eye’s preoperative aberrations without inducing new aberrations postoperatively, unlike standard LASIK profiles which induce spherical aberrations.
Topography-Guided LASIK - calculates the elevation profile from the preoperative corneal topography and corrected corneal surfaces is modeled to eliminate refractive error and higher order aberrations. The difference between the two surfaces forms the basis for the ablation profile.
Aspheric or Q-Factor-Adjusted LASIK - uses the Q-factor or asphericity of the preoperative cornea to calculate the amount of tissue removal needed to reach the optimum Q-factor (-0.4).